3M AbThera Open Abdomen Negative Pressure Therapy

How AbThera Therapy works
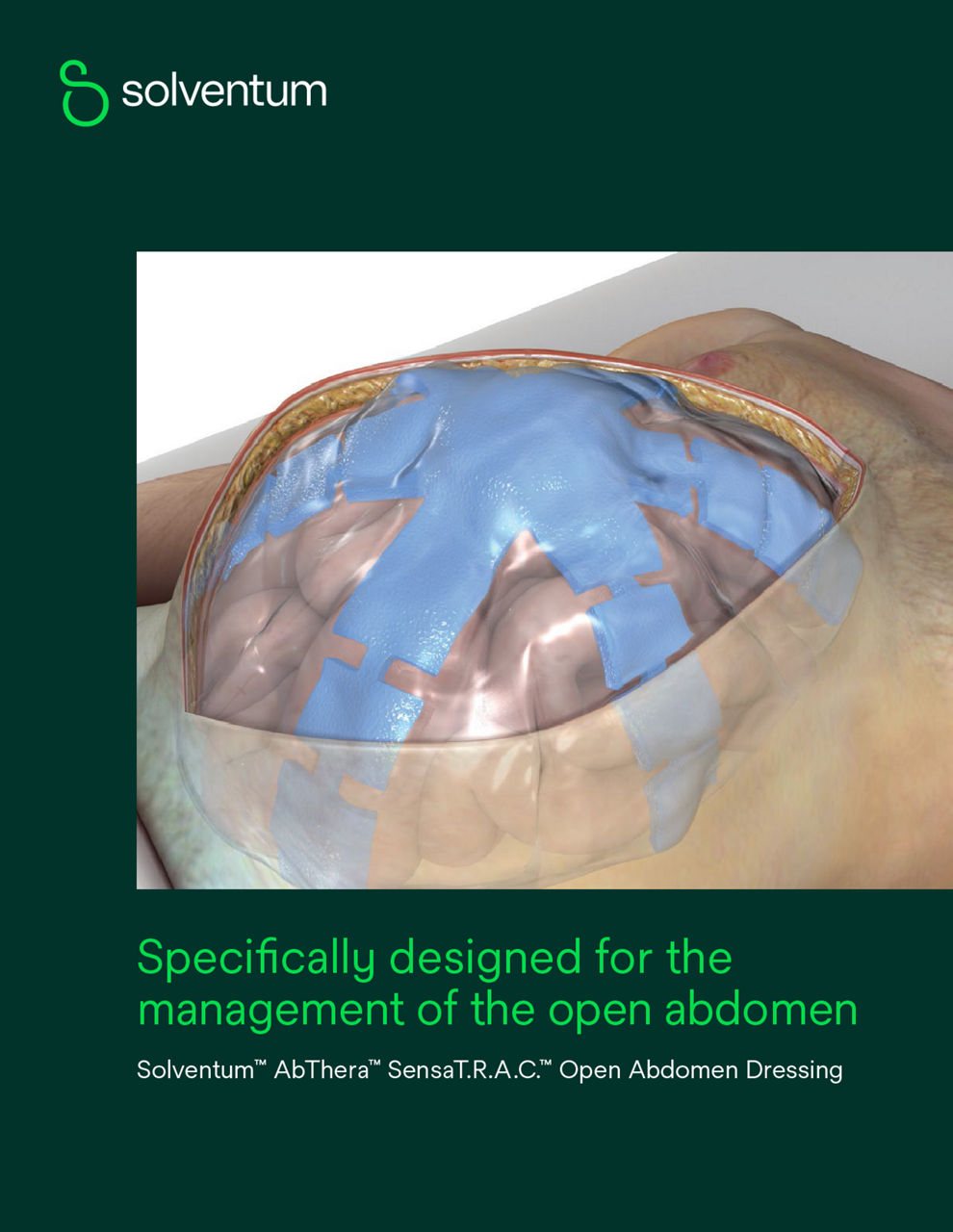
AbThera Therapy is a temporary abdominal closure system designed for simplicity, ease of use, and fast application.1 It uses continuous negative pressure to remove fluids from the abdominal cavity and draw wound edges together, helping to achieve primary fascial closure while protecting abdominal contents from external contamination. The system features a visceral protective layer with encapsulated foam to help remove fluid.
Abdominal closure case study
See the real-world impact of AbThera Therapy
Find out why surgeons choose AbThera Therapy and the AbThera Advanced Dressing to help close abdominal fascial wounds.
The challenge
A 24-year-old female presented to the Emergency Department with complaints of abdominal and back pain, dizziness and near syncopal episode. She was noted as afebrile, tachycardic (140 beats per minute [bpm]), and hypotensive (systolic in the 60’s mmHg). On physical examination, she had left lower quadrant tenderness.
A continuous wave, obstetrical Doppler ultrasound revealed an early intrauterine pregnancy (11-week gestation) and a fetal heart rate of 135 bpm. She had leukocytosis (18.9%) and a neutrophil count of 84% - 10^9.
Ringer’s lactate solution was administered intravenously for her hypotension, and she remained tachycardic (> 120 bpm). A Focused Assessment with Sonography for Trauma (FAST) detected free fluid in the pelvis and right upper quadrant.
The patient was anemic (hemoglobin = 6.8 -g/dl), which raised concern for intraabdominal bleeding of unknown origin and prompted a general surgery consult. An abdominal computed tomography (CT) scan revealed dilated loops of small bowel but diffuse thickness consistent with edema and a fluid-filled abdominopelvic cavity. Given her hemodynamic instability and CT scan, she was taken to the operating room (OR) for diagnostic laparoscopy.
 + patient in supine position (B)")
A) AbThera Advance Dressing placement after small bowel resection (patient in supine position)
B) AbThera Advance Dressing placement after small bowel resection.
Patient data and photos courtesy of Marc R. Matthews, MD, MS, FACS, Associate Director, Arizona Burn Center, Director, Burn Emergency Services Director, Respiratory Care Services, Maricopa Medical Center.
The solution
The patient underwent diagnostic laparoscopy that was converted to laparotomy. Patient had bloody ascites and loops of necrotic small bowel. An internal hernia defect facilitated volvulization of the small bowel, which required intestinal detorsion and prompted a resection of 300 cm of ischemic small bowel. The bowel was left in discontinuity and 3M™ AbThera™ Advance Open Abdomen Dressing was placed in the open abdomen for temporary closure. On postoperative day 2, the patient returned to the OR for 3M™ AbThera™ Advance Open Abdomen Dressing removal; abdominal lavage; a stapled, jejunal-colonic, end-to-end anastomosis; appendectomy; placement of a nasoenteric tube and fascial closure. She was discharged on hospital day 7. In this case, 3M™ AbThera™ Advance Open Abdomen Dressing helped facilitate fascial closure and helped by actively removing fluid and providing medial tension which facilitates subsequent fascial closure.
AbThera Therapy Dressings
Choose from a range of specialized dressings designed to help surgeons manage different types of open abdominal wounds.


Hear from experts
3M™ AbThera™ Open Abdomen Sepsis Video


Article: Exploring open abdomen therapy
Read this Advances in Wound Care article about managing the open abdomen and selecting an appropriate treatment strategy. The review provides an overview of laparotomy, covers the latest techniques for temporary abdominal closure, such as negative pressure wound therapy (NPWT), and recommends treatment strategies to help manage the open abdomen.
You’ll learn how to:
- Identify patients for temporary abdominal closure
- Implement common strategies to achieve temporary closure
- Select the appropriate treatment option for your patients
- Manage infections and support better healing outcomes
Additional articles
- Treatment of Complex Thoracic and Abdominal Trauma Patientsopens in a new tab
- Are commercial negative pressure systems worth the cost in open abdomen management?opens in a new tab
- Prospective study examining clinical outcomes associated with a negative pressure wound therapy system and Barker's vacuum packing techniqueopens in a new tab
AbThera Therapy application videos
3M™ Abthera™ Therapy on the 3M™ V.A.C.® Ulta 4 Therapy System


Resources
Additional AbThera Therapy case studies
- Use of 3M™ AbThera™ Advance Open Abdomen Dressing following emergent exploratory celiotomy (PDF, 996 K)opens in a new tab
- Temporary abdominal wall closure following severe peritonitis and colonic anastomotic leak (PDF, 996 K)opens in a new tab
- Colon resection fistula (PDF, 996 K)opens in a new tab
- Use of 3M™ AbThera™ Advance Open Abdomen Dressing for definitive closure following a diagnostic laparotomy in a patient with peritonitis and perforated bowel PDF, 996 K)opens in a new tab
- Use of 3M™ AbThera™ Advance Open Abdomen Dressing for abdominal fascial closure following infarcted small bowel removal and subsequent end-to-end anastomosis (PDF, 996 K)opens in a new tab
- Hemorrhagic pancreatitis with ACS (PDF, 996 K)opens in a new tab
- Temporary abdominal wall closure following penetrating trauma (PDF, 996 K)opens in a new tab
- Use of 3M™ AbThera™ Advance Open Abdomen Dressing for definitive abdominal closure following umbilical hernia repair and the resection of a necrotic small bowel (PDF, 996 K)opens in a new tab
- Temporary closure using 3M™ AbThera™ Open Abdomen Negative Pressure Therapy following motor vehicle accidentopens in a new tab
Explore more

NOTE: Specific indications, contraindications, warnings, precautions, and safety information exist for these products and therapies. Please consult a clinician and product instructions for use prior to application. This material is intended for healthcare professionals. Rx only.
References:
1. Cheatham ML, et al. Prospective Study Examining Clinical Outcomes Associated with a Negative Pressure Wound Therapy System and Barker’s Vacuum Packing Technique. World Journal of Surgery. 2013 Sep;37(9):2018-30.
2. Kirkpatrick AW, Roberts DJ, Faris PD et al. Active Negative Pressure Peritoneal Therapy After Abbreviated Laparotomy: The Intraperitoneal Vacuum Randomized Controlled Trial. Ann Surg 2015;262(1):38-46.
3. Atema JJ, Gans SL, Boermaster MA. Systematic Review and Meta-analysis of the Open Abdomen and Temporary Abdominal Closure Techniques in Non-trauma Patients. World J Surg. 2015;39(4):912-925.
4. Fitzpatrick ER. Open abdomen in trauma and critical care. Critical Care Nurse. 2017 Oct 1;37(5):22-45.
5. Schmidt M, Hall C, Mercer D, Kieswetter K. Novel foam design actively draws wound edges together under negative pressure: benchtop and pre-clinical assessment [abstract]Schmidt M, Hall C, Mercer D, Kieswetter K. Presented at the SAWC Fall 2018 Meeting, November 2-4, 2018, Las Vegas, Nevada 2018
6. Frazee RC, Abernathy SW, Jupiter DC, et al. Are Commercial Negative Pressure Systems Worth the Cost in Open Abdomen Management? J Am Coll Surg. 2013 April 1;216(4):730-3
7. Campbell A, Chang M, Fabian T et al. Management of the open abdomen: from initial operation to definitive closure. Am Surg 2009 November 1;75(11 Suppl):S1-S22.